Summary
Clinical characteristics.
Potocki-Lupski syndrome (PTLS) is characterized by cognitive, behavioral, and medical manifestations. Cognitively, most individuals present with developmental delay, later meeting criteria for moderate intellectual disability. Behaviorally, issues with attention, hyperactivity, withdrawal, and anxiety may be seen. Some individuals meet criteria for autism spectrum disorder. Medically, hypotonia, oropharyngeal dysphagia leading to failure to thrive, congenital heart disease, hypoglycemia associated with growth hormone deficiency, and mildly dysmorphic facial features are observed. Medical manifestations typically lead to identification of PTLS in infancy; however, those with only behavioral and cognitive manifestations may be identified in later childhood.
Diagnosis/testing.
The diagnosis of PTLS is established by detection of a heterozygous duplication at chromosome 17p11.2 that encompasses RAI1. A recurrent 3.7-Mb duplication accounts for approximately two thirds of 17p11.2 duplications; approximately one third are non-recurrent duplications that encompass RAI1 and vary in size from 0.41 Mb to 19.7 Mb.
Management.
Treatment of manifestations: A multidisciplinary evaluation involving healthcare providers from multiple specialties varies by the age and presenting issues of each individual. Management of all manifestations of PTLS is per standard care.
Surveillance: Routine monitoring for growth deceleration, short stature, failure to thrive; periodic developmental assessment by a developmental specialist; screen for behavior problems at every visit; consultation with a psychiatrist and/or psychologist if there are behavioral concerns; follow up of congenital heart disease as per cardiac consultant.
Genetic counseling.
PTLS is inherited in an autosomal dominant manner. The majority of affected individuals have a de novo duplication; however, parent-to-child transmission has been reported. If the 17p11.2 duplication identified in the proband is not identified in either parent, the risk for future pregnancies could be slightly greater than that of the general population (though still <1%) because of the possibility of parental somatic and or germline mosaicism for the duplication. If one of the parents has the 17p11.2 duplication, the risk to each sib of inheriting the duplication is 50%. It is not possible to reliably predict the phenotype of individuals who inherit the duplication. Prenatal testing and preimplantation genetic testing using chromosomal microarray (CMA) to detect the 17q11.2 duplication found in the proband are possible.
Diagnosis
Suggestive Findings
Potocki-Lupski syndrome (PTLS) should be suspected in individuals with the following [Potocki et al 2007, Soler-Alfonso et al 2011, Neira-Fresneda & Potocki 2015]:
- Neurodevelopmental findings:
- Mild-to-moderate infantile hypotonia with oropharyngeal dysphagia and failure to thrive
- Developmental delay; intellectual disability (typically moderate)
- Communication disorder with verbal apraxia and abnormalities of intonation and prosody
- Sleep-disordered breathing (most evident on sleep studies)
- Features of autism spectrum disorder; hyperactivity
- Congenital heart disease, typically left ventricular outflow track spectrum and/or rhythm disturbances
- Growth hormone deficiency
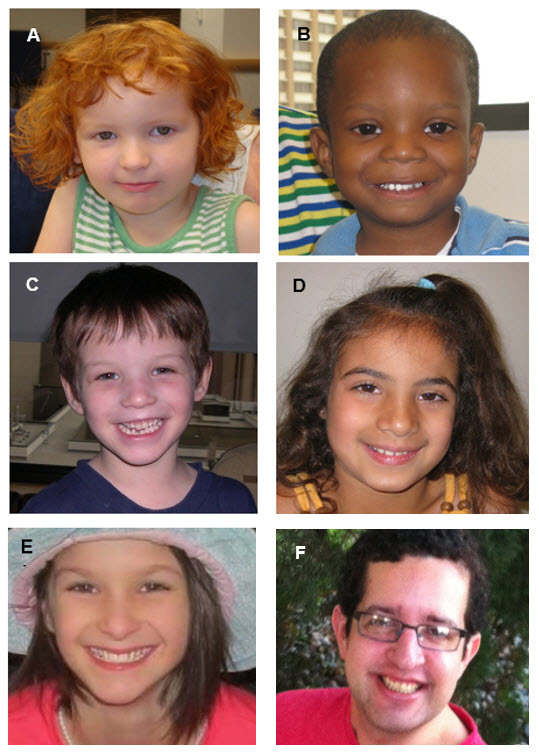
- Mildly to nonspecific dysmorphic facial features [Potocki et al 2007, Neira-Fresneda & Potocki 2015] (see Figure 1).

Figure 1.
Individuals with Potocki-Lupski syndrome. The facial features are not strikingly dysmorphic though common findings include micrognathia (in early childhood) and downslanting palpebral fissures. A. Female age three years ten months
Establishing the Diagnosis
The diagnosis of PTLS is established by detection of a heterozygous duplication at chromosome 17p11.2 that encompasses RAI1 [Potocki et al 2000]. Most individuals with PTLS are identified by chromosomal microarray performed in the context of evaluation for hypotonia, failure to thrive, developmental delay, intellectual disability, or autism spectrum disorder.
For this GeneReview, the 17p11.2 recurrent duplication, observed in approximately two thirds of individuals with PTLS, is defined by a 3.7-Mb duplication at the proximal region of chromosome 17 spanning an approximate interval of 16,757,111-20,219,651 in the reference genome (NCBI Build hg19 genome.ucsc.edu/cgi-bin/hgGateway). Note: Non-recurrent duplications (which encompass RAI1) account for approximately one third of individuals with PTLS and vary in size from 0.41 Mb to 19.7 Mb (see Molecular Pathogenesis).
ISCN nomenclature for the recurrent duplication is: arr[hg19] 17p11.2(16,757,111-20,219,651)x3. Note: Since this duplication is recurrent and mediated by segmental duplications, the unique genetic sequence that is duplicated is the same in all individuals with the syndrome; however, the reported size of the duplication may: (1) be slightly larger or smaller if adjacent segmental duplications are included in the size; and (2) vary based on the design of the microarray used to detect it (see Molecular Pathogenesis).
Although several genes are within the 3.7-Mb recurrent duplication, only RAI1 has been implicated as the dosage-sensitive cause of the phenotype [Bi 2005, Walz et al 2004, Walz et al 2006]. (See Molecular Genetics for genes of interest in the duplicated region.)
The best genomic testing method is chromosomal microarray (CMA) using oligonucleotide or SNP arrays that can detect the recurrent duplication in a proband. The ability to size the duplication depends on the type of microarray used and the density of probes in the 17p11.2 region. Note: (1) This duplication is the reciprocal recombination product of the Smith-Magenis syndrome (SMS) deletion; therefore, this region has been represented since the inception of array CGH technology. (2) Although interphase fluorescent in situ hybridization using RAI1 or high-resolution G-banded chromosome analysis can detect the recurrent 3.7-Mb duplication, these methods are highly dependent on cell preparation and technical skills, and thus lack sensitivity [Potocki et al 2007].
Table 1.
Genomic Testing Used in Potocki-Lupski Syndrome
Clinical Characteristics
Clinical Description
Potocki-Lupski syndrome (PTLS) is characterized by developmental delay, intellectual disability, behavioral disturbances, organ system involvement, and mildly dysmorphic facial features [Potocki et al 2007, Treadwell-Deering et al 2010]. See Figure 1.
PTLS can manifest in infancy with hypotonia, oropharyngeal dysphagia leading to failure to thrive, congenital heart disease, and hypoglycemia associated with growth hormone deficiency. In contrast, individuals who are more mildly affected may manifest cognitive and behavioral abnormalities only, and not be diagnosed until later in childhood [Potocki et al 2007, Treadwell-Deering et al 2010, Neira-Fresneda & Potocki 2015].
Neurodevelopmental
Mild-to-moderate infantile hypotonia with oropharyngeal dysphagia is common and contributes to poor feeding and mild-to-moderate gross motor delays [Potocki et al 2007, Soler-Alfonso et al 2011]. Poor feeding or poor weight gain can be an initial presentation. Infants and children have significantly lower weight for age, weight for length, and BMI for age than the reference population [Soler-Alfonso et al 2011].
Although gross motor delay is observed in the vast majority, most will achieve independent walking by age two years. Rarely, independent ambulation can be delayed until age four years.
Cognitive impairment is one of the most common characteristics of PTLS [Potocki et al 2007]. The vast majority of individuals tested have moderate intellectual disability [Treadwell-Deering et al 2010].
Speech delay is universal. Standardized testing has revealed expressive and receptive language impairment which can include articulation difficulties and disordered intonation and prosody [Treadwell-Deering et al 2010]. Some individuals may exhibit verbal apraxia.
While there are no formal studies of articulation and language abilities in teens and adults with PTLS, verbal abilities appear to improve both with age and speech therapy. Little data regarding findings in adults are available; however, adults with a confirmed molecular genetic diagnosis who have been clinically evaluated have cognitive challenges.
Sleep-disordered breathing. Although sleep disturbances are not often clinically recognized and significant airway obstruction is not found on examination, abnormalities frequently evident on sleep studies include sleep-disordered breathing such as mild central and/or obstructive sleep apnea [Potocki et al 2007, Neira-Fresneda & Potocki 2015]. Children with sleep apnea may present with snoring or hyperactivity. In addition, periodic limb movement disorder is commonly observed.
Behavioral difficulties identified by objective measures and by parental reports include attention problems, withdrawal, and high levels of hyperactivity and anxiety. Reported deficits in executive functioning include initiating and shifting activities and working memory.
Autism spectrum disorder (ASD) and/or autistic features (decreased eye contact, motor mannerisms or posturing, sensory hypersensitivity or preoccupation, repetitive behaviors, difficulty with transitions, lack of appropriate functional or symbolic play, and lack of joint attention) are seen in affected individuals [Potocki et al 2007, Treadwell-Deering et al 2010, Neira-Fresneda & Potocki 2015]. Using validated scoring systems (ADI-R and ADOS-G), Treadwell-Deering et al [2010] found that approximately 60% of a small cohort of children with PTLS met criteria for ASD.
Congenital Heart Disease
Cardiovascular anomalies are reported in about 40% of individuals with PTLS [Potocki et al 2007, Jefferies et al 2012]. The anomalies can include atrial septal defect and ventricular septal defect, as well as anomalies within the left ventricular outflow track spectrum including bicuspid aortic valve, dilated aortic root, and hypoplastic left heart [Sanchez-Valle et al 2011, Yusupov et al 2011, Bravo et al 2013].
A smaller percentage of individuals with PTLS have rhythm disturbances detected on ECG [Jefferies et al 2012].
Growth Hormone Deficiency
Five of seven individuals in the original description of PTLS had short stature; one of the five had documented growth hormone deficiency [Potocki et al 2000]. In a second study, one of ten individuals had short stature (but not growth hormone deficiency) [Potocki et al 2007]. Subsequently, additional individuals with PTLS and growth hormone deficiency have been identified, including some with hypoglycemia in infancy and short stature in early childhood [Author, personal observation].
Other
Musculoskeletal features of PTLS that can mimic those seen in connective tissue disorders include severe bilateral clubfeet [Dhanaraj et al 2015], joint hypermobility, kyphoscoliosis, pes planus, and long fingers and toes [Martin et al 2008].
Renal anomalies include hypoplastic, multicystic dysplastic kidneys, and hydronephrosis [Goh et al 2012].
EEG abnormalities observed during sleep include slow occipital dominant rhythm and generalized and/or focal epileptiform abnormalities. Clinical or electroencephalographic seizures have not been reported [Potocki et al 2007, Neira-Fresneda & Potocki 2015].
Other findings include the following [Potocki et al 2007, Neira-Fresneda & Potocki 2015]:
- Hyperopia (common, but not significant enough to require corrective lenses in childhood)
- Mild high-frequency sensorineural hearing loss
- Dental malocclusion and dental crowding
Penetrance
Penetrance is 100%; expression of phenotypic features is variable.
Prevalence
The prevalence of PTLS is approximately one in 25,000 [Greenberg et al 1991, Liu et al 2011].
Genetically Related Disorders
Yuan-Harel-Lupski (YUHAL) syndrome (OMIM 616652) is caused by a contiguous gene duplication of chromosome 17p12-p11.2 that includes the genes PMP22 (OMIM 601097) and RAI1 (OMIM 607642). This syndrome is a complex neurodevelopmental disorder characterized by developmental delay and early-onset peripheral neuropathy. The disorder comprises features of both demyelinating Charcot-Marie-Tooth disease type 1A (CMT1A; see CMT Overview), caused by duplication of PMP22, and Potocki-Lupski syndrome, caused by duplication of a slightly proximal region on 17p11.2 that includes RAI1 [Yuan et al 2015].
Differential Diagnosis
The differential diagnosis of Potocki-Lupski syndrome (PTLS) is broad due to the wide spectrum of findings and presence of developmental delay, learning problems, and neuropsychiatric disorders – for which the differential diagnosis is extensive. All manifestations of PTLS can also be seen individually or in combination in individuals with other genomic disorders.
Management
Evaluations and Referrals Following Initial Diagnosis
To establish the extent of disease and needs in an individual diagnosed with Potocki-Lupski syndrome (PTLS), the evaluations and referrals summarized in Table 2 (if not performed as part of the evaluation that led to diagnosis) are recommended.
Note: Some evaluations are age dependent and may not be relevant at the time of initial diagnosis (e.g., recommendation for cognitive testing for intellectual disability during infancy).
Table 2.
Recommended Evaluations and Referrals Following Initial Diagnosis of Potocki-Lupski Syndrome
Treatment of Manifestations
Depending on the age and presenting problems of the individual with PTLS, a multidisciplinary evaluation involving healthcare providers from the following specialties is often necessary: audiology, cardiology, dental, developmental pediatrics, endocrinology, feeding, gastroenterology, general pediatrics, clinical genetics, ophthalmology, orthopedics, otolaryngology, physical medicine and rehabilitation, psychiatry, sleep medicine, speech pathology, and urology.
Table 3.
Treatment of Medical Manifestations in Individuals with PTLS
Developmental Delay / Intellectual Disability Management Issues
The following information represents typical management recommendations for individuals with developmental delay/intellectual disability in the United States; standard recommendations may vary from country to country.
Ages 0-3 years. Referral to an early intervention program is recommended for access to occupational, physical, speech, and feeding therapy. In the US, early intervention is a nationwide federally funded program available in all states.
Ages 3-5 years. In the US, developmental preschool through the local public school district is recommended. A "full individual evaluation" (FIE) will occur before placement to determine needed services and therapies and will be subsequently integrated into an individualized education plan (IEP).
Ages 5-21 years
- In the US, an IEP based on the individual’s level of function should be developed by the local public school district. Affected children are permitted to remain in the public school district generally until age 21.
- Discussion about transition plans including medical and financial guardianship, financial, vocation/employment, and medical arrangements should begin at age 12 years. Developmental pediatricians can provide assistance with transition to adulthood.
All ages. Consultation with a developmental pediatrician is recommended to ensure the involvement of appropriate community, state, and educational agencies and to support parents in maximizing quality of life.
Consideration of private supportive therapies based on the affected individual's needs is recommended. Specific recommendations regarding type of therapy can be made by a developmental pediatrician.
In the US:
- Developmental Disabilities Administration (DDA) enrollment is recommended. DDA is a public agency that provides services and support to qualified individuals. Eligibility differs by state but is typically determined by diagnosis and/or associated cognitive/adaptive disabilities.
- Families with limited income and resources may also qualify for supplemental security income (SSI) for their child with a disability.
Motor Dysfunction
Gross motor dysfunction
- Physical therapy is recommended to maximize strength and mobility and to reduce the risk for later-onset orthopedic complications (e.g., scoliosis). Aquatic therapy and hippotherapy (therapeutic horseback riding) may also be considered.
- Consider use of durable medical equipment as needed (e.g., orthotics, adaptive strollers).Physical medicine and rehabilitation evaluations may be warranted [Neira-Fresneda & Potocki 2015].
Fine motor dysfunction. Occupational therapy is recommended to address difficulty with fine motor skills that affect adaptive function such as feeding, grooming, dressing, and handwriting.
Oral motor dysfunction. Feeding therapy, typically from an occupational or speech therapist, is recommended for affected individuals who have difficulty feeding due to poor oral motor control and/or sensory aversions, assuming the individual is safe to eat by mouth.
Communication issues. Consider:
- Speech and language therapy to address receptive and expressive language deficits, articulation abnormalities, and verbal apraxia;
- Evaluation for alternative means of communication (e.g., Augmentative and Alternative Communication) for individuals who have expressive language difficulties.
Social/Behavioral Concerns
Children may qualify for and benefit from interventions used in treatment of autism spectrum disorder, including applied behavior analysis (ABA). ABA therapy is targeted to the individual child’s behavioral, social, and adaptive strengths and weaknesses and is typically performed one on one with a board-certified behavior analyst.
Consultation with a developmental pediatrician may be helpful in guiding parents through appropriate behavior management strategies or providing prescription medications when necessary.
Surveillance
Table 4.
Recommended Surveillance for Individuals with PTLS
Evaluation of Relatives at Risk
See Genetic Counseling for issues related to testing of at-risk relatives for genetic counseling purposes.
Therapies Under Investigation
Search ClinicalTrials.gov in the US and EU Clinical Trials Register in Europe for access to information on clinical studies for a wide range of diseases and conditions. Note: There may not be clinical trials for this disorder.
Genetic Counseling
Genetic counseling is the process of providing individuals and families with information on the nature, mode(s) of inheritance, and implications of genetic disorders to help them make informed medical and personal decisions. The following section deals with genetic risk assessment and the use of family history and genetic testing to clarify genetic status for family members; it is not meant to address all personal, cultural, or ethical issues that may arise or to substitute for consultation with a genetics professional. —ED.
Mode of Inheritance
Potocki-Lupski syndrome (PTLS) is inherited in an autosomal dominant manner. The majority of affected individuals have a de novo duplication; however, parent-to-child transmission has been reported [Magoulas et al 2014].
Risk to Family Members
Parents of a proband
- Evaluation of the parents by genomic testing that will detect the 17p11.2 duplication present in the proband is recommended.
- Although not described to date, there is a theoretic (though unlikely) possibility that a parent could have somatic mosaicism for the 17p11.2 duplication.
- Note: A parent who manifests only cognitive and behavioral abnormalities may not be diagnosed with PTLS until the birth of an affected child (see Clinical Description).
Sibs of a proband. The risk to the sibs of the proband depends on the genetic status of the parents:
- If the 17p11.2 duplication identified in the proband is not identified in either parent, the empiric recurrence risk to sibs is approximately 1% because of the theoretic possibility of parental germline mosaicism [Campbell et al 2015].
- If one of the parents has the 17p11.2 duplication, the risk to each sib of inheriting the duplication is 50%. It is not possible to reliably predict the phenotype of individuals who inherit the duplication.
Offspring of a proband. Offspring of an individual with the 17p11.2 duplication have a 50% chance of inheriting the duplication. It is not possible to reliably predict the exact phenotype of the individual; however, the clinical features detailed in Clinical Description would be expected.
Other family members. The risk to other family members depends on the genetic status of the proband’s parents: if a parent has the 17p11.2 duplication, his or her family members may also have the duplication.
Related Genetic Counseling Issues
Family planning
- The optimal time for determination of genetic risk and discussion of the availability of prenatal/preimplantation genetic testing is before pregnancy. Similarly, decisions about testing to determine the genetic status of at-risk apparently asymptomatic family members are best made before pregnancy.
- It is appropriate to offer genetic counseling (including discussion of potential risks to offspring and reproductive options) to young adults who are at risk of having a child with 17p11.2 duplication.
DNA banking is the storage of DNA (typically extracted from white blood cells) for possible future use. Because it is likely that testing methodology and our understanding of genes, allelic variants, and diseases will improve in the future, consideration should be given to banking DNA of affected individuals.
Prenatal Testing and Preimplantation Genetic Testing
Pregnancies known to be at increased risk for the 17p11.2 duplication. Prenatal and preimplantation genetic testing using chromosomal microarray (CMA) to detect the 17q11.2 duplication found in the proband may be offered when:
- A parent has the 17p11.2 duplication;
- Neither parent has the duplication but has had a child with the 17p11.2 duplication. In this instance, the recurrence risk associated with the possibility of parental germline mosaicism or other predisposing genetic mechanisms is approximately 1%.
Differences in perspective may exist among medical professionals and within families regarding the use of prenatal testing, particularly if the testing is being considered for the purpose of pregnancy termination rather than early diagnosis. While most centers would consider use of prenatal testing to be a personal decision, discussion of these issues may be helpful.
Pregnancies not known to be at increased risk for the 17p11.2 duplication. CMA performed in a pregnancy not known to be at increased risk for PTLS may detect the duplication.
Note: Regardless of whether a pregnancy is known or not known to be at increased risk for Potocki-Lupski syndrome, prenatal genetic testing results cannot reliably predict the phenotype.
Resources
GeneReviews staff has selected the following disease-specific and/or umbrella support organizations and/or registries for the benefit of individuals with this disorder and their families. GeneReviews is not responsible for the information provided by other organizations. For information on selection criteria, click here.
- Potocki-Lupski Syndrome Outreach FoundationPhone: 214-435-8288Email: info@PTLSFoundation.org
- PTLS Hope Research Foundation
Molecular Genetics
Information in the Molecular Genetics and OMIM tables may differ from that elsewhere in the GeneReview: tables may contain more recent information. —ED.
Table A.
Potocki-Lupski Syndrome: Genes and Databases
Table B.
OMIM Entries for Potocki-Lupski Syndrome (View All in OMIM)
Molecular Pathogenesis
Duplication mechanism. The proximal short arm of chromosome 17 is enriched with low-copy repeats (LCRs, also called segmental duplications). The 3.7-Mb recurrent 17p11.2 duplication is the result of nonallelic homologous recombination (NAHR) between homologous, directly oriented LCRs flanking the recurrent duplication region [Park et al 2002, Stankiewicz & Lupski 2010].
NAHR-mediated unequal crossover between other LCRs at the 17p11.2 region results in a less commonly observed ~5-Mb recurrent duplication [Zhang et al 2010]. Non-recurrent duplications overlapping 17p11.2 that are associated with PTLS have also been observed. It has been proposed that replication-based mechanisms, such as fork stalling and template switching/microhomology-mediated break-induced replication (FoSTeS/MMBIR), generate rearrangements independent of LCRs [Hastings et al 2009, Zhang et al 2009]. Replication-based mechanisms may generate larger duplications that encompass both the PTLS critical region at 17p11.2 and the neighboring CMT1A critical region at 17p12, thereby leading to Yuan-Harel-Lupski (YUHAL) syndrome (see Genetically Related Disorders, OMIM 616652, Yuan et al [2015]).
Genes of interest in this region
- RAI1. All PTLS-associated duplications identified to date include the gene RAI1 on chromosome 17p [Zhang et al 2010]. Although the recurrent duplication encompasses about 70 genes, the smallest region of overlap among non-recurrent duplications resulting in the PTLS phenotype is 125 kb and includes only RAI1 [Zhang et al 2010].Moreover, using a transgenic mouse model, a Dp(11)17 allele (duplication of the region on mouse chromosome 11 that is syntenic to human PTLS region) and a null Rai1 allele in compound heterozygous configuration rescues the phenotypes observed in heterozygous Dp(11)17 mice by maintaining normal disomic Rai1 dosage. Moreover, the phenotype observed in Dp(11)17 mice was rescued in Dp(11)17/Rai1(-) despite altered trisomic copy number of the other genes within the region [Walz et al 2006]. This evidence suggests that duplication of RAI1 is sufficient to cause the phenotype.
- FLCN. Folliculin, encoded by FLCN, is highly expressed in kidney. FLCN loss-of-function variants have been reported in Birt-Hogg-Dubé syndrome.Comparison between the duplication segments in PTLS with renal phenotype and the syntenic duplication in mouse model suggests FLCN as a potential contributor to the renal abnormalities [Goh et al 2012].
References
Literature Cited
- Bi W. Inactivation of Rai1 in mice recapitulates phenotypes observed in chromosome engineered mouse models for Smith-Magenis syndrome. Hum Mol Genet. 2005;14:983–95. [PubMed: 15746153]
- Bravo C, Gámez F, Pérez R, Águarón A, De León-Luis J. Prenatal diagnosis of Potocki-Lupski syndrome in a fetus with hypoplastic left heart and aberrant right subclavian artery. J Perinatol. 2013;33:394–6. [PubMed: 23624966]
- Campbell IM, Shaw CA, Stankiewicz P, Lupski JR. Somatic mosaicism: implications for disease and transmission genetics. Trends Genet. 2015;31:382–92. [PMC free article: PMC4490042] [PubMed: 25910407]
- Dhanaraj D, Chu A, Pappas JG, Moran E, Lehman WB. Potocki-Lupski syndrome in conjunction with bilateral clubfoot. J Pediatr Orthop B. 2015;24:373–6. [PubMed: 25768679]
- Goh ES-Y, Perez IC, Canales CP, Ruiz P, Agatep R, Yoon G, Chitayat D, Dror Y, Shago M, Goobie S, Sgro M, Walz K, Mendoza-Londono R. Definition of a critical genetic interval related to kidney abnormalities in the Potocki-Lupski syndrome. Am J Med Genet A. 2012;158A:1579–88. [PubMed: 22639462]
- Greenberg F, Guzzetta V, Montes de Oca-Luna R, Magenis RE, Smith ACM, Lupski JR. Molecular analysis of the Smith-Magenis syndrome: a possible contiguous-gene syndrome associated with del(l7)(pl 1.2). Am J Hum Genet. 1991;49:1207–18. [PMC free article: PMC1686451] [PubMed: 1746552]
- Hastings PJ, Lupski JR, Rosenberg SM, Ira G. Mechanisms of change in gene copy number. Nat Rev Genet. 2009;10:551–64. [PMC free article: PMC2864001] [PubMed: 19597530]
- Jefferies JL, Pignatelli RH, Martinez HR, Robbins-Furman PJ, Liu P, Gu W, Lupski JR, Potocki L. Cardiovascular findings in duplication 17p11.2 syndrome. Genet Med. 2012;14:90–4. [PMC free article: PMC3666919] [PubMed: 22237436]
- Liu P, Lacaria M, Zhang F, Withers M, Hastings PJ, Lupski JR. Frequency of nonallelic homologous recombination is correlated with length of homology: evidence that ectopic synapsis precedes ectopic crossing-over. Am J Hum Genet. 2011;89:580–8. [PMC free article: PMC3188830] [PubMed: 21981782]
- Magoulas PL, Liu P, Gelowani V, Soler-Alfonso C, Kivuva EC, Lupski JR, Potocki L. Inherited dup(17)(p11.2p11.2): expanding the phenotype of the Potocki-Lupski syndrome. Am J Med Genet A. 2014;164A:500–4. [PubMed: 24311450]
- Martin J, Knight SJL, Sharp AJ, Eichler EE, Hurst J, Kini U. Potocki-Lupski syndrome mimicking a connective tissue disorder. Clin Dysmorph. 2008;17:211–3. [PubMed: 18541972]
- Neira-Fresneda J, Potocki L. Neurodevelopmental disorders associated with abnormal gene dosage: Smith-Magenis and Potocki-Lupski Syndromes. J Pediatr Genet. 2015;4:159–67. [PMC free article: PMC4918721] [PubMed: 27617127]
- Park SS, Stankiewicz P, Bi W, Shaw C, Lehoczky J, Dewar K, Birren B, Lupski JR. Structure and evolution of the Smith-Magenis syndrome repeat gene clusters, SMS-REPs. Genome Res. 2002;12:729–38. [PMC free article: PMC186597] [PubMed: 11997339]
- Potocki L, Bi W, Treadwell-Deering D, Carvalho CMB, Eifert A, Friedman EM, Glaze D, Krull K, Lee JA, Lewis RA, Mendoza-Londono R, Robbins-Furman P, Shaw C, Shi X, Weissenberger G, Withers M, Yatsenko SA, Zackai EH, Stankiewicz P, Lupski JR. Characterization of Potocki-Lupski syndrome (dup(17)(p11.2p11.2)) and delineation of a dosage-sensitive critical interval that can convey an autism Phenotype. Am J Hum Genet. 2007;80:633–49. [PMC free article: PMC1852712] [PubMed: 17357070]
- Potocki L, Chen K-S, Park S-S, Osterholm DE, Withers MA, Kimonis V, Summers AM, Meschino WS, Anyane-Yeboa K, Kashork CD, Shaffer LG, Lupski JR. Molecular mechanism for duplication 17p11.2 - the homologous recombination reciprocal of the Smith-Magenis microdeletion. Nat Genet. 2000;24:84–7. [PubMed: 10615134]
- Sanchez-Valle A, Pierpont ME, Potocki L. The severe end of the spectrum. Hypoplastic left heart in Potocki-Lupski syndrome. Am J Med Genet A. 2011;155A:363–6. [PMC free article: PMC3092288] [PubMed: 21271655]
- Soler-Alfonso C, Motil KJ, Turk CL, Robbins-Furman P, Friedman EM, Zhang F, Lupski JR, Fraley JK, Potocki L. Potocki-Lupski syndrome: A microduplication syndrome associated with oropharyngeal dysphagia and failure to thrive. J Pediatr. 2011;158:655–9.e2. [PMC free article: PMC3059370] [PubMed: 21168152]
- Stankiewicz P, Lupski JR. Structural variation in the human genome and its role in disease. Ann Rev Med. 2010;61:437–55. [PubMed: 20059347]
- Treadwell-Deering DE, Powell MP, Potocki L. Cognitive and behavioral characterization of the Potocki-Lupski syndrome (duplication 17p11.2). J Dev Behav Pediatr. 2010;31:137–43. [PubMed: 20110824]
- Walz K, Paylor R, Yan J, Bi W, Lupski JR. Rai1 duplication causes physical and behavioral phenotypes in a mouse model of dup(17)(p11.2p11.2). J Clin Invest. 2006;116:3035–41. [PMC free article: PMC1590269] [PubMed: 17024248]
- Walz K, Spencer C, Kaasik K, Lee CC, Lupski JR, Paylor R. Behavioral characterization of mouse models for Smith-Magenis syndrome and dup(17)(p11.2p11.2). Hum Mol Genet. 2004;13:367–78. [PubMed: 14709593]
- Yuan B, Harel T, Gu S, Liu P, Burglen L, Chantot-Bastaraud S, Gelowani V, Beck CR, Carvalho CMB, Cheung SW, Coe A, Malan V, Munnich A, Magoulas PL, Potocki L, Lupski JR. Nonrecurrent 17p11.2p12 rearrangement events that result in two concomitant genomic disorders: the PMP22-RAI1 contiguous gene duplication syndrome. Am J Hum Genet. 2015;97:691–707. [PMC free article: PMC4667131] [PubMed: 26544804]
- Yusupov R, Roberts AE, Lacro RV, Sandstrom M, Ligon AH. Potocki-Lupski syndrome: An inherited dup(17)(p11.2p11.2) with hypoplastic left heart. Am J Med Genet A. 2011;155A:367–71. [PubMed: 21271656]
- Zhang F, Khajavi M, Connolly AM, Towne CF, Batish SD, Lupski JR. The DNA replication FoSTeS/MMBIR mechanism can generate genomic, genic and exonic complex rearrangements in humans. Nat Genet. 2009;41:849–53. [PMC free article: PMC4461229] [PubMed: 19543269]
- Zhang F, Potocki L, Sampson JB, Liu P, Sanchez-Valle A, Robbins-Furman P, Navarro AD, Wheeler PG, Spence JE, Brasington CK, Withers MA, Lupski JR. Identification of uncommon recurrent Potocki-Lupski syndrome-associated duplications and the distribution of rearrangement types and mechanisms in PTLS. Am J Hum Genet. 2010;86:462–70. [PMC free article: PMC2833368] [PubMed: 20188345]
Chapter Notes
Revision History
- 24 August 2017 (bp) Review posted live
- 10 October 2016 (jn) Original submission
Publication Details
Author Information and Affiliations
Houston, Texas
Houston, Texas
Houston, Texas
Publication History
Initial Posting: August 24, 2017.
Copyright
GeneReviews® chapters are owned by the University of Washington. Permission is hereby granted to reproduce, distribute, and translate copies of content materials for noncommercial research purposes only, provided that (i) credit for source (http://www.genereviews.org/) and copyright (© 1993-2024 University of Washington) are included with each copy; (ii) a link to the original material is provided whenever the material is published elsewhere on the Web; and (iii) reproducers, distributors, and/or translators comply with the GeneReviews® Copyright Notice and Usage Disclaimer. No further modifications are allowed. For clarity, excerpts of GeneReviews chapters for use in lab reports and clinic notes are a permitted use.
For more information, see the GeneReviews® Copyright Notice and Usage Disclaimer.
For questions regarding permissions or whether a specified use is allowed, contact: ude.wu@tssamda.
Publisher
University of Washington, Seattle, Seattle (WA)
NLM Citation
Potocki L, Neira-Fresneda J, Yuan B. Potocki-Lupski Syndrome. 2017 Aug 24. In: Adam MP, Feldman J, Mirzaa GM, et al., editors. GeneReviews® [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2024.